“We’ve Got You, Ms. Evelyn”: A Story of Remote Patient Monitoring in Action
By Kelli Stovall, RPh. EMBA
VP of Pharmacy Services and Clinical Programs
Published: May 8, 2025

Let me tell you about Ms. Evelyn.
Ms. Evelyn has lived in the same rural community her whole life, raised three kids, and worked part-time at the library until just a few years ago. Recently widowed, she now lives alone in her small farmhouse outside of town. She still makes her own bread (from scratch!) and tends to her garden every day.
But life has gotten a bit harder lately.
When Evelyn was discharged from the hospital last month, she had a lot going on, heart failure, diabetes, and high blood pressure. Her doctors did their best to explain everything before she left, but the truth is, she went home overwhelmed and exhausted. Her discharge papers filled an entire folder, her medications changed completely, and her doctor asked her to come back for follow-ups within the next week.
There was just one problem: Ms. Evelyn no longer drives. Due to her health conditions, she made the decision to stop driving when she turned 78. Her daughter lives out of state, and her nearest family is a cousin about an hour away. Her next-door neighbor and friend always offer to give rides into town, but she often hesitates to ask.
She told the pharmacist all this when she called to check on her.
You see, Evelyn’s doctor referred her to the local pharmacy for remote patient monitoring after she was discharged from the hospital. They knew she was high-risk and wanted to make sure someone could keep an eye on her vital signs from home.
So, they got her set up.
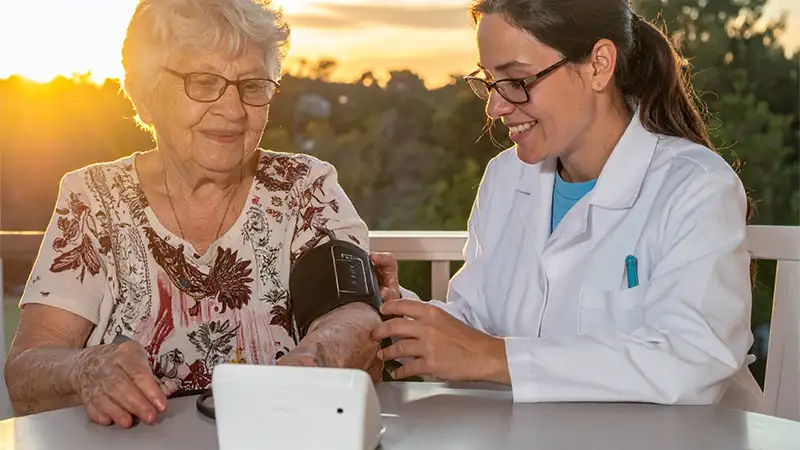
One of the pharmacy techs, Angela, drove out to Evelyn’s house with a kit: a simple blood pressure cuff, a weight scale, and a pulse oximeter, that could transmit readings automatically. No internet? No problem. These devices came with built-in cellular. Angela walked her through each device slowly, while sitting on the front porch as the sun sat low on the horizon, casting a warm glow across the sky, and made sure Evelyn felt comfortable before she left.
That first week, Evelyn’s blood pressure readings were okay… until they weren’t.
One morning, her numbers were way up, and she had gained three pounds overnight. By morning, her oxygen level started to dip. All of this happened before Evelyn even realized anything was wrong.
But because the pharmacist was reviewing her vitals in real-time, they caught it.
The pharmacist gave her a call. Ms. Evelyn said she hadn’t been feeling quite right, just more tired than usual, but figured it was just part of recovering. The pharmacist then coordinated with her cardiologist, and her meds were adjusted. Ms. Evelyn avoided what could have been a serious situation. No ER visit. No 911 call. No hospital readmission.
Just support. Just care.
When they checked in with her a week later, Evelyn said, “I sleep better knowing someone’s watching. I don’t feel so alone anymore.”

Bridging the Gap with Pharmacy at Home Care: How Community Pharmacies Can Use Remote Patient Monitoring to Support Patients After Hospital Discharge
If you work in a community pharmacy, or even if you’re just passionate about improving healthcare, you’ve probably noticed the same thing I have: too many patients fall through the cracks after they leave the hospital. They’re sent home with a stack of discharge papers, new medications, and a long list of “dos and don’ts.” It’s overwhelming, even for the most health-literate folks. And for those juggling chronic
conditions or lacking support at home, it’s a setup for a readmission.
That’s where remote patient monitoring (RPM) comes in. And yes, it absolutely belongs in a community pharmacy setting. This is why remote patient monitoring in community pharmacies is such a big deal for patients recently discharged from the hospital.
It’s not just technology. It’s not just billing codes and vitals. It’s real people, like Evelyn, who want to stay safe and independent in their own homes, even when life gets complicated.
And it’s about us, community pharmacists, being the bridge between the hospital and home. Especially for those who don’t have easy access to transportation or nearby family, we might be the closest support they’ve got.
Why Transitions of Care Matter
Transitions of care (TOC) refer to the critical period when a patient moves from one care setting to another, most commonly, from the hospital to home. This is when a lot can go wrong: meds get missed, follow-ups are delayed, and warning signs go unnoticed.
Here’s the kicker: most hospital readmissions happen within 30 days of discharge, and many of them are preventable.
Imagine if we could check in on our patients in real time during this window. Imagine if we could catch a sudden blood pressure spike or notice a 5-pound weight gain that signals fluid retention. That’s the power of RPM.
Implementing RPM in a Community Pharmacy: Let’s Break It Down
Okay, so how do we actually do this in a pharmacy setting? Here’s a roadmap:
1. Identify Your Target Population
Start with patients at high risk for readmission, think heart failure, COPD, hypertension, and diabetes. Work with local providers or health systems to identify recently discharged patients who could benefit from RPM. Proactively share information with community providers so they can build your services into a comprehensive discharge plan.
2. Partner with a Technology Vendor
You don’t need to reinvent the wheel. There are RPM platforms designed specifically for pharmacies. Look for one that offers user-friendly devices, seamless data transmission, and a dashboard that makes monitoring easy for your staff.
3. Train Your Team
Your technicians and pharmacists will need some training to support RPM workflows. That might include device setup, patient education, and interpreting the incoming data. But don’t worry, it’s very doable. Many vendors offer onboarding support.
4. Educate Your Patients
Help patients understand the “why” behind RPM. Let them know it’s not just about numbers; it’s about having a healthcare partner who’s watching out for them when they need it most. Set clear expectations and make sure they’re comfortable using the devices.
5. Monitor, Engage, and Intervene
Once the data starts flowing in, your team can flag concerns, follow up with the patient, and even notify their provider if needed. Combine this with medication reconciliation and adherence support, and you’ve got a powerful transition of care model.

Let’s Talk Dollars: Who Pays for RPM?
Now, I know what you’re probably thinking: “This sounds great, but how do we actually get paid for it?” Fair question!
RPM is reimbursable, and the coverage is growing fast.
Medicare covers RPM services, and as of December 2023, 37 state Medicaid programs are on board.
By winter 2024, 42 states were offering some form of RPM reimbursement in their Medicaid programs. That’s nearly double what it was just a few years ago.
And here’s something cool, some states like Louisiana are stepping up and requiring all private insurers operating in the state to cover RPM in some form.
Plus, an increasing number of commercial payers are getting on the RPM train.
Just be aware that coverage can vary. Some states only pay if RPM is delivered through a home health agency, or they limit what conditions or types of monitoring qualify. So it’s worth checking your state’s Medicaid policies or partnering with someone who knows the landscape.
How Is RPM Reimbursed?
Here’s a quick breakdown:
Initial patient enrollment and setup (including device setup and education) is reimbursable under CPT code 99453.
You’ll receive a monthly base payment for managing the device and reviewing patient data.
There’s also additional reimbursement available for time spent managing care. You can bill for each 20-minute increment (up to 60 minutes) using CPT code 99457 and 99458. And yes, clinical staff can provide those care management services.
It’s not a fortune, but it adds up, especially when layered into your existing workflow. Plus, it’s a way to offer real value to your patients and stand out in a crowded pharmacy market.
Real Talk: Does This Actually Help?
YES. Studies show that remote monitoring can reduce hospital readmissions, improve medication adherence, and help patients feel more supported. But you don’t need a journal article to see the value, you’ll feel it when a patient tells you, “I didn’t have to go back to the ER because you caught it in time.”

The Big Picture
Community pharmacies are already doing so much to close care gaps. Implementing remote patient monitoring for newly discharged patients just takes it a step further. It’s about being more than a pharmacy; it’s about being a lifeline.
So, if you’ve ever wished you could do more for your patients after they leave the hospital, now’s your chance. RPM gives us the tools. Let’s use them.
Want to dive deeper into billing codes or discuss RPM tech platforms that work best for pharmacies? We’d be happy to help you navigate the details. Let’s chat and build something great for your community!
Sources
While the story of Ms. Evelyn is fictional, the blog content is informed by real-world sources, data, and policies. Here’s a list of sources and references that support the factual elements discussed:
- Center for Connected Health Policy (CCHP)
- Information on Medicaid RPM reimbursement and state-by-state policy differences.
- https://www.cchpca.org
- Centers for Medicare & Medicaid Services (CMS)
- CPT codes and RPM reimbursement policies under Medicare.
- https://www.cms.gov
- American Medical Association (AMA) CPT® Codes
- CPT Code 99453 (device setup and patient education)
- CPT Code 99454 (device supply and data transmission)
- CPT Code 99457/99458 (20- and 40-minute RPM care management billing)
- https://www.ama-assn.org
- Louisiana Department of Insurance
- Mandates regarding private payer RPM coverage within the state.
- https://www.ldi.la.gov
- American Heart Association & Journal of Telemedicine and Telecare
- Evidence supporting RPM’s effectiveness in reducing hospital readmissions and improving chronic disease management.
- National Rural Health Association (NRHA)
- Context for rural healthcare access issues and transportation barriers post-discharge.
- https://www.ruralhealthweb.org
- OpenAI
- OpenAI. (2025). ChatGPT (April 29 version) [Large language model].
- https://chat.openai.com/